Musculoskeletal modelling in Spine Surgery
This project aims at using multi-rigid body musculoskeletal modelling for meaningful functional analysis of patients afflicted with spine pathologies.
Multi-rigid body musculoskeletal modelling lends itself well for an efficient and integral, yet detailed, analysis of the biomechanical state of the healthy, pathological (adjacent segment disease, spondylolisthesis, scoliosis, etc.) and instrumented human spine during movement (Figure 1). With the use of inverse kinematics and static optimization, joint loads and muscle forces can be computed (Figure 2). It has been shown that properties such as spinopelvic alignment, weight, and height affect the loading at intervertebral joints, highlighting the importance of patient-specific models. Both subject-specificity and automation of model creation are necessary for the successful transfer into an orthopaedic clinical workflow. In addition to valuable direct information about spine loading, the output of a robust musculoskeletal model can be used to further enhance patient-specificity in other modelling modalities by providing valuable boundary conditions. For example, transferring kinematics-dependent muscle forces and joint reaction forces to (subject-specific) FE models allows more physiological loading conditions and therefore a supposedly improved structural analysis through the latter simulation approach.
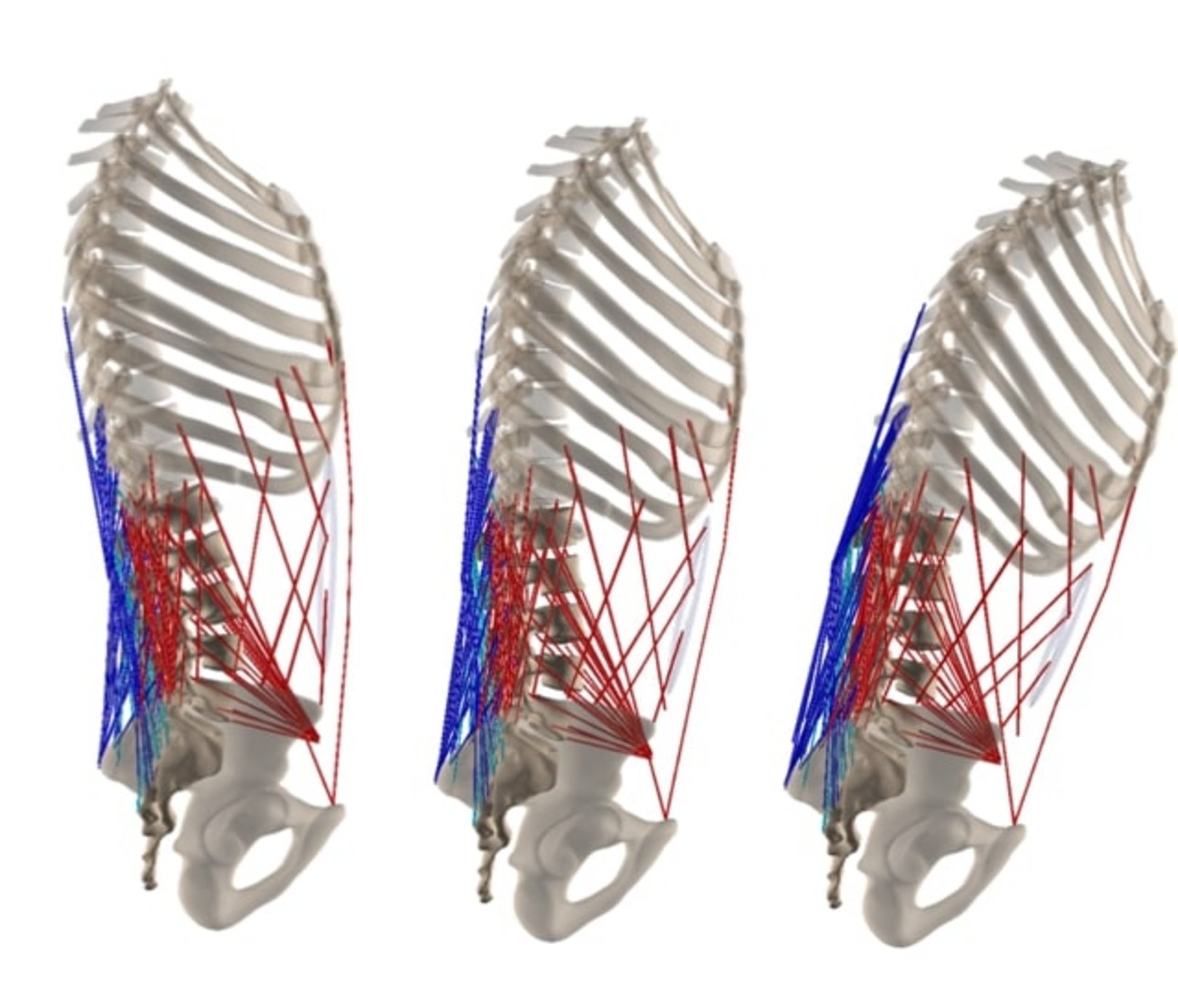
Figure 1: Musculoskeletal model in extended, neutral, and flexed position.
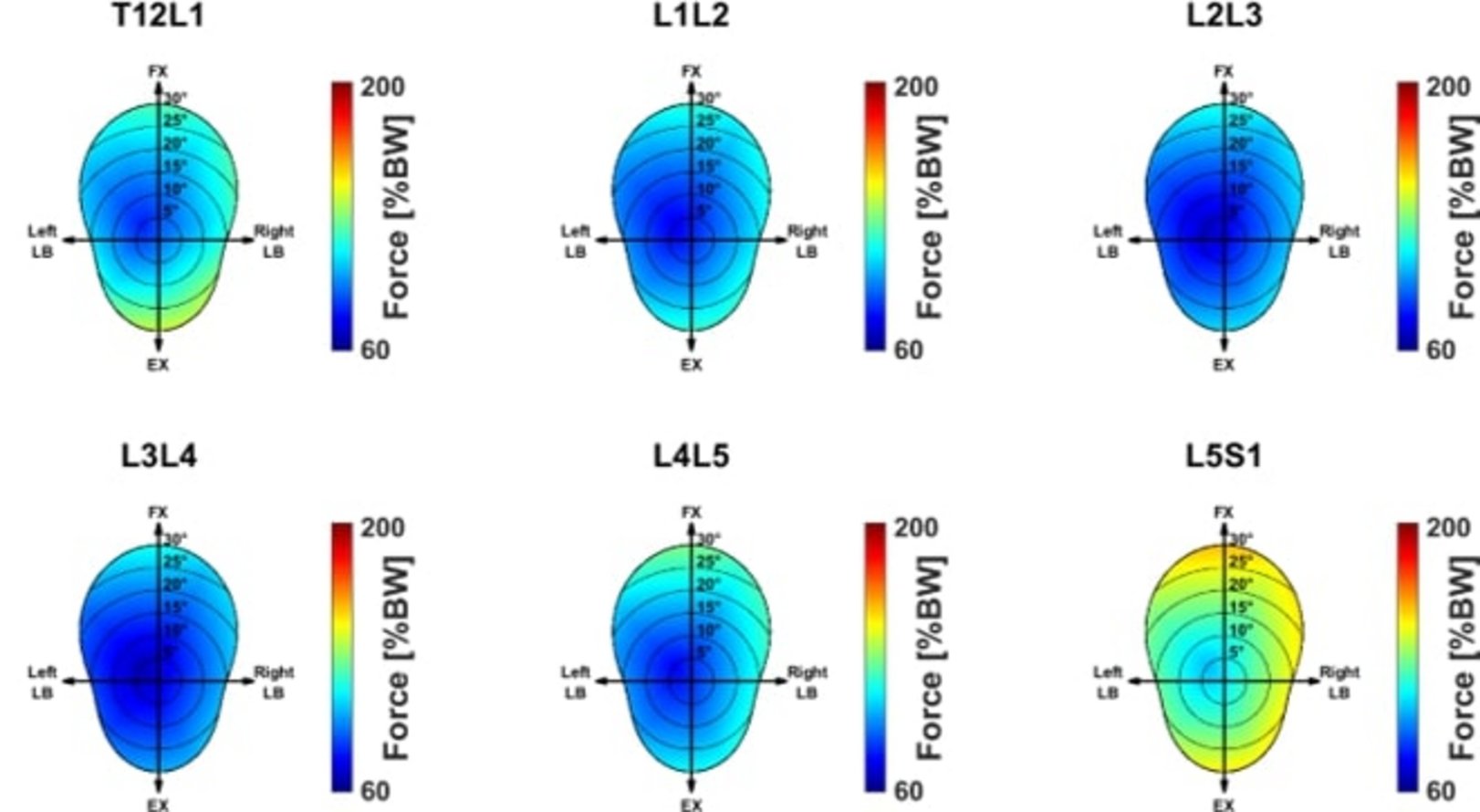
Figure 2: Heat map representation of joint reaction forces in the lumbosacral joints normalized by body weight.
We have developed an automated pipeline for the creation of semi-patient-specific musculoskeletal models. The model represents the anatomy and alignment of the spine, reflects the patient's mass distribution, and allows the optimization target to be varied. Patient information can be obtained and incorporated using computed tomography images and/or frontal and lateral X-rays (EOS) of the spine.
Spinal fusion is the gold standard for treating a variety of pathologies affecting the spine. With regard to preoperative planning, we will investigate the use of musculoskeletal models to determine optimized fusion angles by attempting to minimize joint loads. ASD often occurs after spinal fusion and can lead to neurological symptoms and pain. The etiology of the disease is still controversial, and a variety of factors are associated with it. One suspected cause is increased and unusual stress and movement above and below the fused segment. Retrospective musculoskeletal modeling and analysis of patients with and without postoperative ASD is a promising approach to evaluate whether altered biomechanics are involved in the pathogenesis of ASD.


